 This past weekend, I attended the 9th Annual Joining FORCEs Against Hereditary Breast and Ovarian Cancer Conference in Philadelphia. This is the only event of its kind; created by and for the members of the HBOC community. To say that this event was awesome is a gross understatement. It was an amazing weekend packed with relevant content and activities.
This past weekend, I attended the 9th Annual Joining FORCEs Against Hereditary Breast and Ovarian Cancer Conference in Philadelphia. This is the only event of its kind; created by and for the members of the HBOC community. To say that this event was awesome is a gross understatement. It was an amazing weekend packed with relevant content and activities.
Leading researchers and experts in related fields presented on latest research. I learned about newest options for cancer screening and prevention. Most interesting to me were the sessions related to ovarian cancer, since I am currently considering a risk-reducing bilateral salpingo-oophorectomy (BSO).
My personal takeaways on the topic of Ovarian Cancer: Early Detection and Prevention, presented by Dr. Beth Karlan, Cedars-Sinai (slides):
- Taking tubes only (salpingectomy) and sparing the ovaries is a reasonable intermediate step for younger women (I’m 34). It is still recommended to remove the ovaries in natural menopausal age (early 50s).
- Taking one ovary does not change age of menopause.
- In general, there is no need to remove uterus at time of BSO or salpingectomy alone, based on current info and this varies by individual.
The tube-only and one ovary option is very attractive to me at this point. However, if I choose the BSO, surgical menopause will very shortly follow, so I also attended a session about Managing Menopause Without Hormones by Dr. Ann Steiner, Penn (slides) and Dr. Diljeet Singh, Permanente (slides). If you’ve been reading my blog for a bit, you may have noticed that I maintain a plant-based lifestyle and stay away from processed or synthetic products. When it comes to managing menopause symptoms with hormone replacement therapy (HRT), I am hesitant. I understand there are bio-identical hormones available and Premarin is an option, but I am uncomfortable with the idea of any HRT, because essentially I will be introducing something my body didn’t produce itself naturally/synthetic. After this great session about other options for managing symptoms, I stuck around to ask each of these experts their opinion on HRT for someone like me, who will need to be on it for 10+ years. Would they recommend HRT to manage long-term issues (osteoporosis, heart disease, loss of cognitive function, etc.) or can these symptoms be successfully managed without HRT? I didn’t get a clear answer and the advice was conflicting, so the jury is still out. If I choose to spare an ovary or both, this will be a non-issue, but nonetheless it was great to learn about the non-HRT options.
I will be discussing this topic again with my gyn onc in October, when it is time for my bi-annual screening (TVU and CA-125). At this time, I know I will be having some risk-reducing surgery in the future, but have not yet decided which type and when.
 One of t
One of t he other awesome things about the conference is that many other women (and men) from our relatively small HBOC community attend (650 this year), so it’s an opportunity to finally meet in-person some individuals I’ve been chatting with online. Also, got a chance to catch up with those that were there last year. Loved spending time with my FORCE buds!
he other awesome things about the conference is that many other women (and men) from our relatively small HBOC community attend (650 this year), so it’s an opportunity to finally meet in-person some individuals I’ve been chatting with online. Also, got a chance to catch up with those that were there last year. Loved spending time with my FORCE buds!
And lastly, THANK YOU FOR YOUR SUPPORT to all those that came to visit nope2BC and bought jewelry. All the proceeds are donated to FORCE and with your help, we raised a lot of money! Hope you enjoy your pieces.
Will you join us next year? The 10th Annual Joining FORCEs Against Hereditary Breast and Ovarian Cancer Conference will take place in Orlando, FL, October 6-8, 2016. I’ll be there!


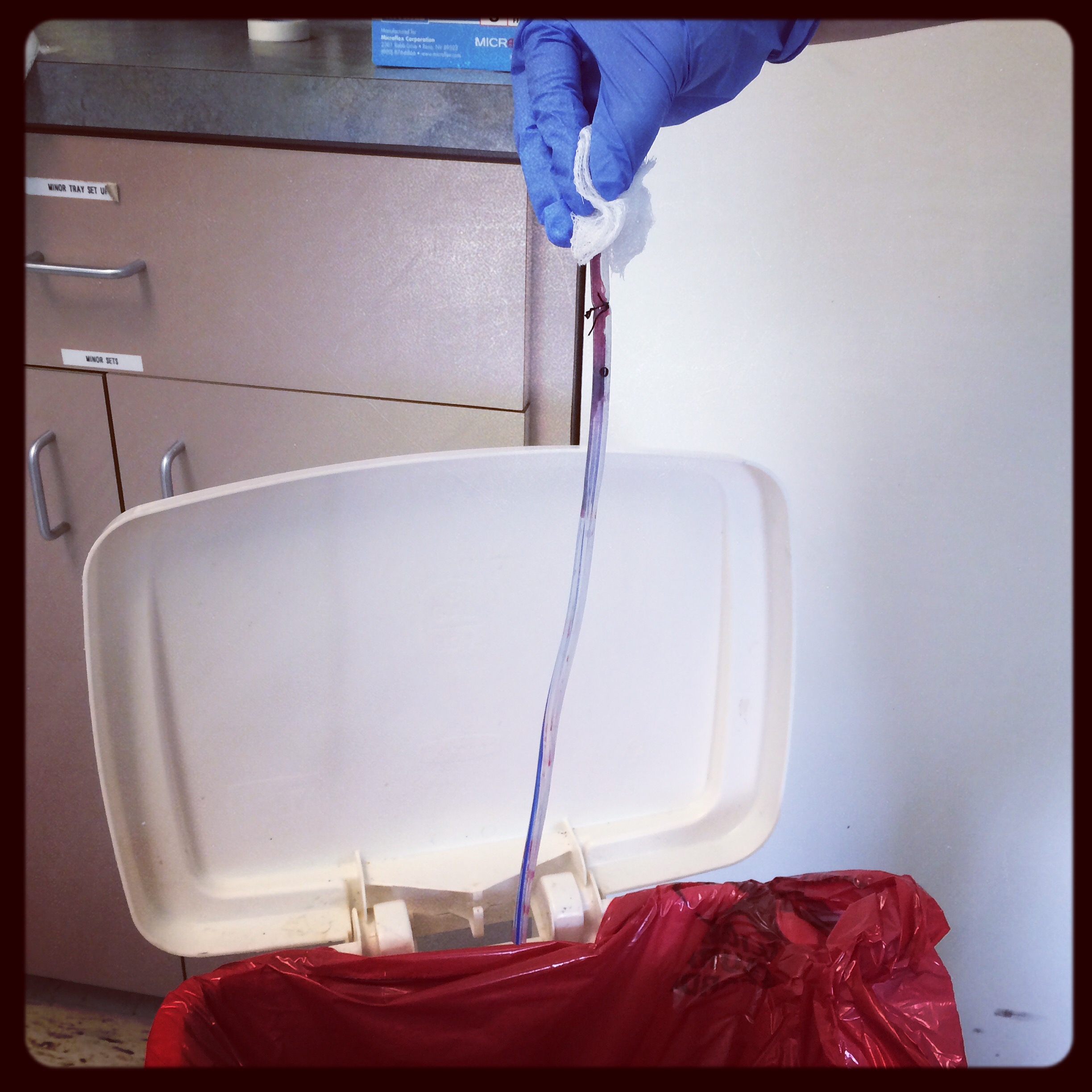 Although my level of activity was low, drain output was 80mL for the first couple of days, so it had to stay in a bit longer. During my second follow up appointment, on Monday, the drain was removed. About a foot of tubing, which was placed in the pocket around the implant, was pulled out (see pic on right: from the black stitch just under the hand, all the way down!). This is usually not painful, just weird. Good riddance! Feeling so much better with that thing out of me. Dr. M declared that things were looking good and ordered a follow up a week later.
Although my level of activity was low, drain output was 80mL for the first couple of days, so it had to stay in a bit longer. During my second follow up appointment, on Monday, the drain was removed. About a foot of tubing, which was placed in the pocket around the implant, was pulled out (see pic on right: from the black stitch just under the hand, all the way down!). This is usually not painful, just weird. Good riddance! Feeling so much better with that thing out of me. Dr. M declared that things were looking good and ordered a follow up a week later.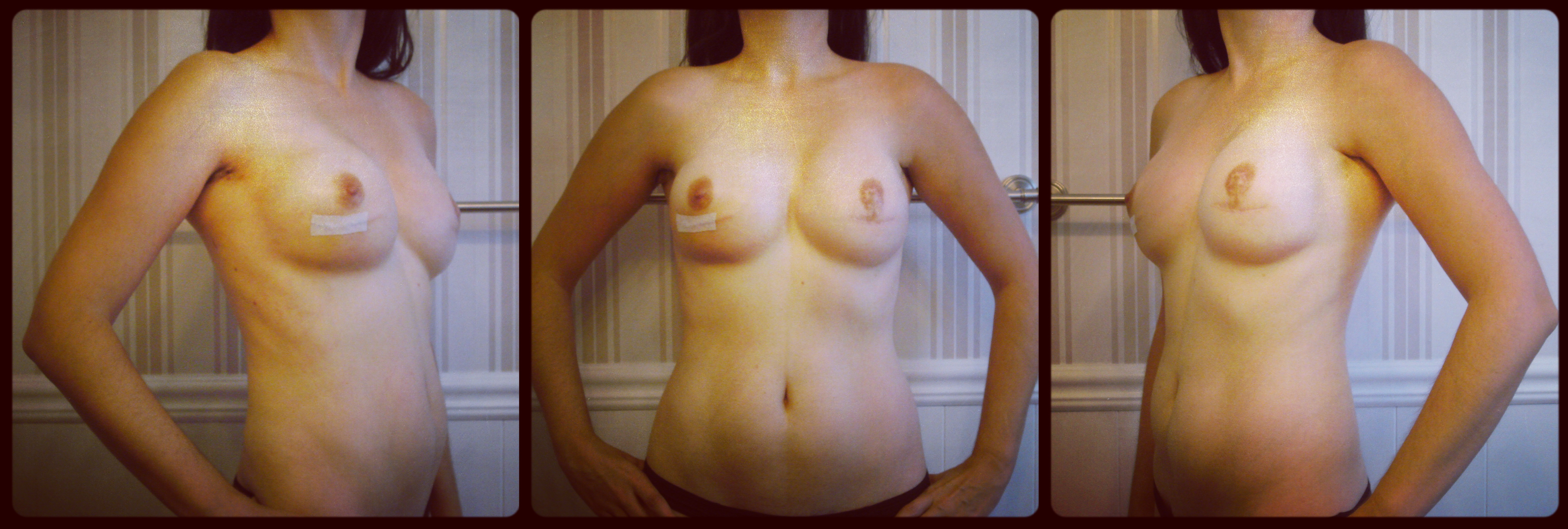
 I am still swollen and bruised (Arnica helped), but the result is pretty darn good, considering the circumstances. I’m hesitant to celebrate, however. With my history, I have a few more weeks to go until I can breathe a little easier. The issues I experienced after my last two exchange surgeries (see: Houston, we have a problem and Déjà vu) both happened about a month out. So, fingers crossed that this is my happy ending! I can’t wait to move on with my life.
I am still swollen and bruised (Arnica helped), but the result is pretty darn good, considering the circumstances. I’m hesitant to celebrate, however. With my history, I have a few more weeks to go until I can breathe a little easier. The issues I experienced after my last two exchange surgeries (see: Houston, we have a problem and Déjà vu) both happened about a month out. So, fingers crossed that this is my happy ending! I can’t wait to move on with my life.



 Once again, the HBOC community is buzzing. If you haven’t already seen, Angelina Jolie Pitt has published another
Once again, the HBOC community is buzzing. If you haven’t already seen, Angelina Jolie Pitt has published another  Tissue expanders, which are like “pre-implants” (pictured on left), are inserted underneath the
Tissue expanders, which are like “pre-implants” (pictured on left), are inserted underneath the 

 The topic of insurance coverage has come up a bit in the Facebook groups recently. There were some good questions. Having been through a few (ha!) surgeries, appealing rejected claims, and recently switching from one provider to another (United Healthcare > Blue Cross Blue Shield), I have a little bit of experience dealing with insurance and can share some thoughts and things to consider.
The topic of insurance coverage has come up a bit in the Facebook groups recently. There were some good questions. Having been through a few (ha!) surgeries, appealing rejected claims, and recently switching from one provider to another (United Healthcare > Blue Cross Blue Shield), I have a little bit of experience dealing with insurance and can share some thoughts and things to consider.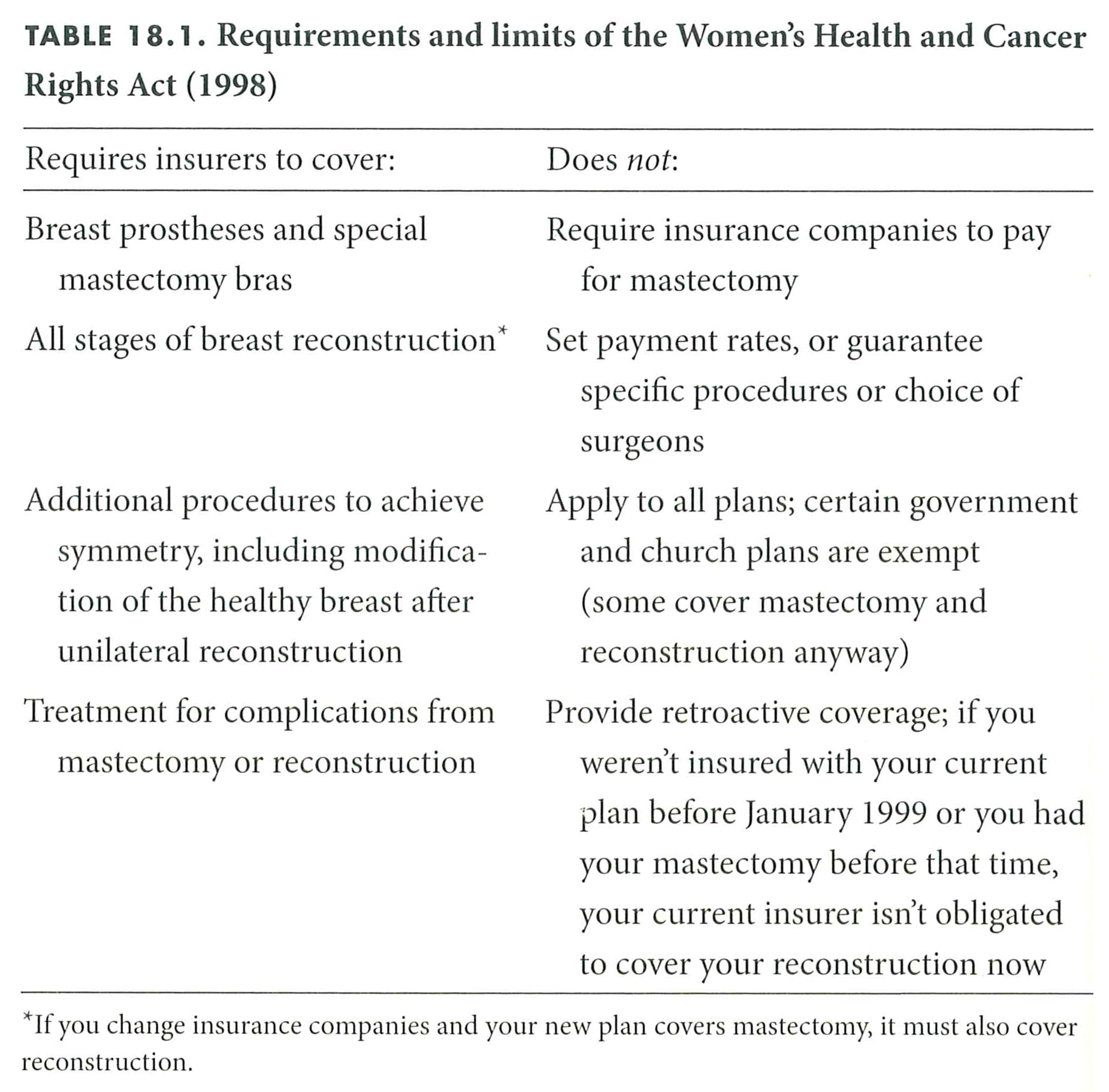







 So far, so good. Things are looking good and healing well after my latest surgery two weeks ago when a tissue expander was placed on my right side. I am not loving the discomfort I have. Feeling no pain, but the tightness is definitely there! It is that elephant-on-your-chest feeling. Not as bad as after original mastectomy, but still very uncomfortable.
So far, so good. Things are looking good and healing well after my latest surgery two weeks ago when a tissue expander was placed on my right side. I am not loving the discomfort I have. Feeling no pain, but the tightness is definitely there! It is that elephant-on-your-chest feeling. Not as bad as after original mastectomy, but still very uncomfortable.
