 Once again, the HBOC community is buzzing. If you haven’t already seen, Angelina Jolie Pitt has published another NY Times Op-Ed. This time about her choice and reasons for undergoing a bilateral salpingo-oophorectomy (removal of fallopian tubes and ovaries). She explains that she has been planning to have this procedure for some time, but recent test results pushed her to go through with it to reduce her risk.
Once again, the HBOC community is buzzing. If you haven’t already seen, Angelina Jolie Pitt has published another NY Times Op-Ed. This time about her choice and reasons for undergoing a bilateral salpingo-oophorectomy (removal of fallopian tubes and ovaries). She explains that she has been planning to have this procedure for some time, but recent test results pushed her to go through with it to reduce her risk.
She is careful to point out that this choice is her own and right for her after carefully considering options, but may not be for others. Surgery is not the only option.
I did not do this solely because I carry the BRCA1 gene mutation, and I want other women to hear this. A positive BRCA test does not mean a leap to surgery. I have spoken to many doctors, surgeons and naturopaths. There are other options. Some women take birth control pills or rely on alternative medicines combined with frequent checks. There is more than one way to deal with any health issue. The most important thing is to learn about the options and choose what is right for you personally.
I am again so thankful that she chose to share with the world her genetic status and decisions related to her health. She is bringing global awareness to hereditary breast and ovarian cancer, what many organizations have been striving to do for years. Also empowering women and families facing hereditary cancer to discuss and seek out options available to them.
As I read and react to her piece, I think of my own family history and my health. I lost my mother to ovarian cancer a little over a year ago (29 year old sister to breast, great grandmother to ovarian, and have an aunt undergoing treatment for colorectal). We do not carry any of the known genetic mutations that increase risk of cancer (we are uninformed negative; read old post on the topic), however, my doctors and genetic counselor are convinced something is there, just hasn’t yet been identified. I am managing my healthcare assuming same. In just a few days I will be meeting with my oncologist for the regular bi-annual appointment, which will include the same blood test Jolie Pitt mentions as well as an ultrasound. I know that just like her, the moment those results are abnormal, my surgery will be scheduled. I have also done lots of research and considered other options, but already know this surgery is the right answer for me personally. It will greatly reduce the risk of ovarian cancer, just as the prophylactic mastectomy does for breast cancer. When is the question. I dread the aftermath, which includes surgical menopause, and have thus far been putting it off. Cross your fingers for me.
For more information about genetic mutations, hereditary breast and ovarian cancer syndrome, screening and prevention options, local support group finder, and much more, visit the FORCE: Facing Our Risk of Cancer Empowered website. Talk to your doctor about your family history and whether genetic testing is right for you. To find a genetic counselor in your area, check the National Society of Genetic Counselors website.







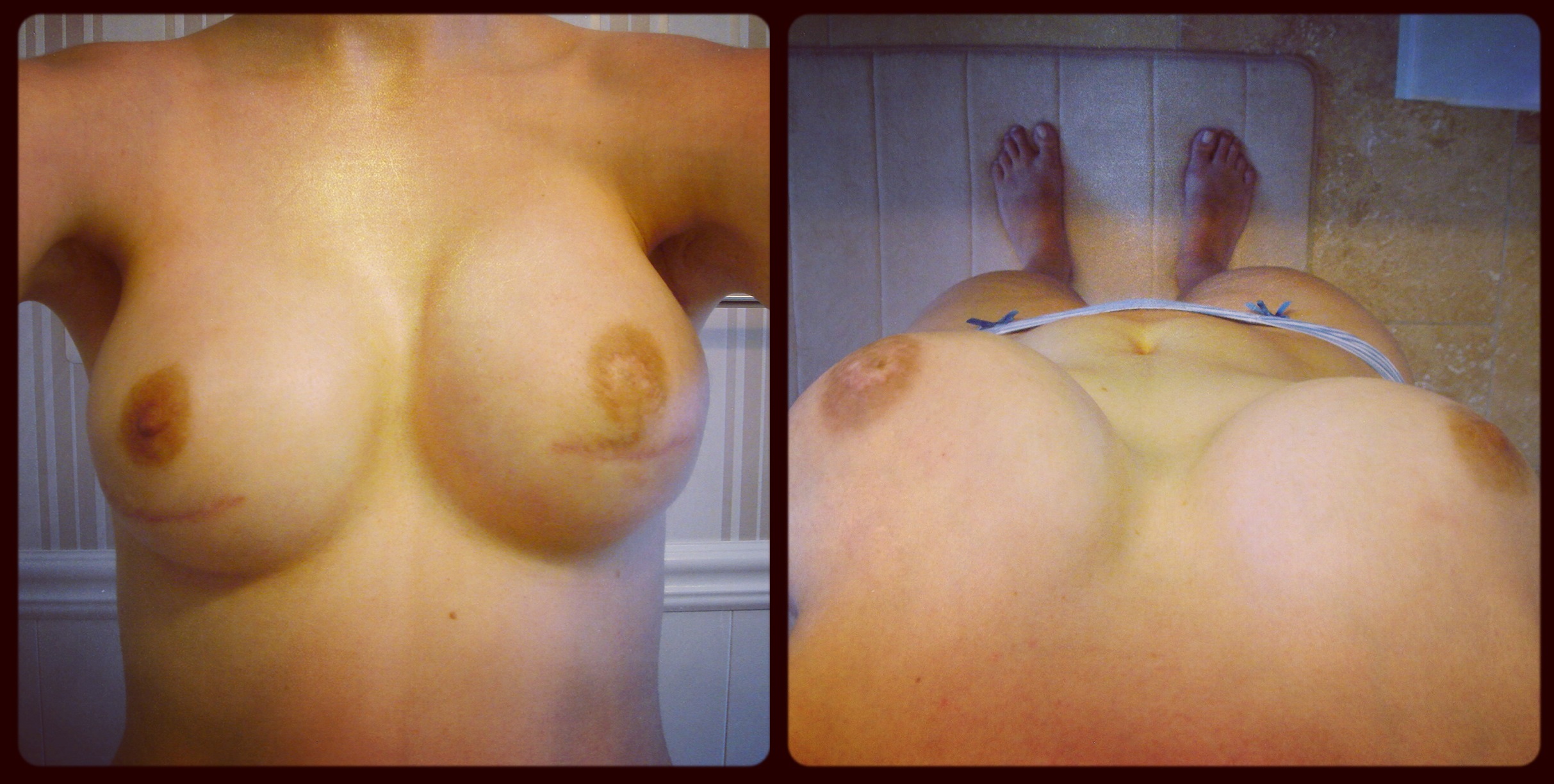





 Breast skin is fragile after mastectomy. If it’s exceptionally thin after the breast tissue is cut away or is handled too roughly, it may die. The same result may occur if the breast surgeon severs too many blood vessels that feed the skin or uses eletrocautery too aggressively and burns the inside of the skin, which may then blister and die.
Breast skin is fragile after mastectomy. If it’s exceptionally thin after the breast tissue is cut away or is handled too roughly, it may die. The same result may occur if the breast surgeon severs too many blood vessels that feed the skin or uses eletrocautery too aggressively and burns the inside of the skin, which may then blister and die. For a recap of why/how the expansion process works, see
For a recap of why/how the expansion process works, see 
 Hyperbaric oxygen therapy (HBOT) involves the breathing of pure oxygen while in a sealed chamber that has been pressurized at 1-1/2 to 3 times normal atmospheric pressure. –
Hyperbaric oxygen therapy (HBOT) involves the breathing of pure oxygen while in a sealed chamber that has been pressurized at 1-1/2 to 3 times normal atmospheric pressure. – 



