Only two weeks to go until my exchange surgery! I am so excited. Can’t wait to be on the other side of this thing. I’m looking forward to being finished. I report to the hospital at 7:30am, for a 9:30am surgery, on Tuesday, September 3rd.
Pre-op appointment
Met with Dr. M this afternoon for my pre-op appointment. Discussed a few more details, got my pictures taken, signed the familiar consent forms, got the don’t-take-these-meds sheet, had my blood drawn, and peed in a cup.
Here are a few of my final questions:
Will I be required to wear any type of bra (compressions or underwire) after the exchange surgery? Should I purchase something? No. If any type of compression is needed it will be via ace bandage and dressings or a mastectomy bra that will be issued by the hospital.
I have hypertrophic-ish spots on my incision scars from the mastectomy, should I use something special after the exchange to prevent this from happening? The lumpy scar tissue will be removed during the exchange surgery. Since the pockets are already created/expanded, there won’t be as much stress on the incisions going forward. Silicone sheets? That’s an option that will apply pressure to the incisions to keep them flat. We will revisit once they close.
What about this ugly, scarred tissue from the area that was necrotic? Depending on how much skin is loose/available after the implants are placed, we may be able to remove the chunk now. Otherwise, a skin graft from the hip area is an option, but that would need to happen at a later time.
And the most important question: will I have drains again? Yes. That wiped the smile off my face. Noooooooooooo! I was hoping I would never see a surgical drain again.
For my photo session today, I removed everything except my underpants. This is the third set of full body pics we’ve taken, but it was still weird. While standing on a pedestal I was thinking of this XKCD strip Lannis shared a little while ago and giggling. Where are my beads? I earned them!
Saline versus silicone? Teardrop or round? Will high profile give enough projection? Choosing implants has been a popular topic in the Prophylactic Mastectomy Facebook group this week. While reviewing feedback of some of the other Ladies, I found myself questioning the choices I’ve made. After looking over my little list yet again, I reaffirmed that I have made the best decision for me. Here are the winners and the losers .
Disclaimer: Each person may give different levels of importance to the factors I list below and should discuss their options with their plastic surgeon. It is not my intention to convey that choosing anything different than what I chose is wrong. I am just presenting my logic. Right, wrong, or just plain stupid. 🙂 As always, I welcome your feedback!
Implant type
Factor
Saline
Silicone
Durability
Incision size
Chance of rippling
Natural feel
Sloshing
Leak detection
All the hoopla about the link between silicone implants and connective tissue disease, breast cancer, or reproductive issues is just that .. hoopla and unproven. It still caused the moratorium on use of silicone implants in the US in 1992, though. Because of this, breast implants are the most tested medical device out there. The moratorium was lifted in 2006. See FDA’s Update on the Safety of Silicone Gel-Filled Breast Implants for more details.
In any case, both types of implants are encased in a silicone shell. The one encasing the silicone implant is solid, but the saline one has a port (salines are inserted deflated and filled with fluid; silicones are pre-filled). Also, salines are more prone to ripple, causing folds in the shell. These two vulnerabilities are the causes of higher failure rates of saline implants. Although they come out on the bottom here, problems with silicone implants are more difficult to detect. Regular MRI screenings for “silent ruptures” are recommended for patients with these types of implants.
On the aesthetic side of the equation, the incisions needed for salines are smaller, but they are firmer and have been reported to produce a “sloshing” noise.
Implant shape
Factor
Round
Anatomical
Natural appearance
Natural feel/motion
Higher projection
Complication due to turning
From the various photos I have seen, I am not convinced that there is much difference in the aesthetic outcome, but in my head it makes more sense that anatomical (teardrop) implants have a more natural shape, so I gave them the . While both shapes are filled with cohesive gel, the degree of viscosity varies between the round and teardrop versions. Teardrops may look better, but they are firmer due to the gel being more form-stable (read: solid). This consistency is what gives the implants the “gummy bear” moniker.
Whether saline or silicone, implants come not only in different shapes, but also either smooth or textured surfaces, as well as different projections. Due to the distribution of the gel within the implant shell, the same volume of silicone produces a higher projection in a round implant versus a teardrop one. The higher the projection, the narrower the base. With a 29″ rib cage, I need narrow implants and the round version offers the highest projection: ultra high.
And lastly, the fact that corrective surgery is required if the implant turns is a big one for me. When a round implant turns, you can’t tell, but if a teardrop is loose within its pocket, it is obvious. With the current state of my expanders (one sits higher than the other), I am nervous about this possible issue and want to avoid it.
So there you have it: I chose round silicone implants.
Check out this awesome video showing the difference between regular round silicone implants and their anatomical counterparts.
This is a video of me playing with a round implant that has been ruptured. You can see that this type of implant is also cohesive enough to not leak outside of the shell. It retracts just as the anatomical implant in the above video.
Total hospital stay after my prophylactic bilateral mastectomy was just a tad over two days. I was not up to or interested in any friends/other family visiting while I was there. Sitting up in bed was challenging and exhausting enough.
The morning of discharge, I saw both surgeons, had a few more hospital staff visitors, and got the discharge paperwork. Prior to surgery I made a list of questions we had to get answered before leaving the hospital, so we gathered the info:
How and when do I empty the drains? A nurse demonstrated how to do this properly. The drains need to be emptied at least twice per day.
Do I need to change the dressings? No, leave as is until the follow up appointment and further instructions from the plastic surgeon.
When is my follow up appointment? Friday morning (3 days post-op).
Can I shower? Not right away. Take a sponge bath or use baby wipes, until told otherwise.
Who do I contact in case of emergency or if I have questions after-hours? Call the plastic surgeon’s office. If after-hours, the answering service knows how to reach him.
When do I get the pathology results? They will be available in about a week. Make an appointment with the breast surgeon.
Pink Passion gown
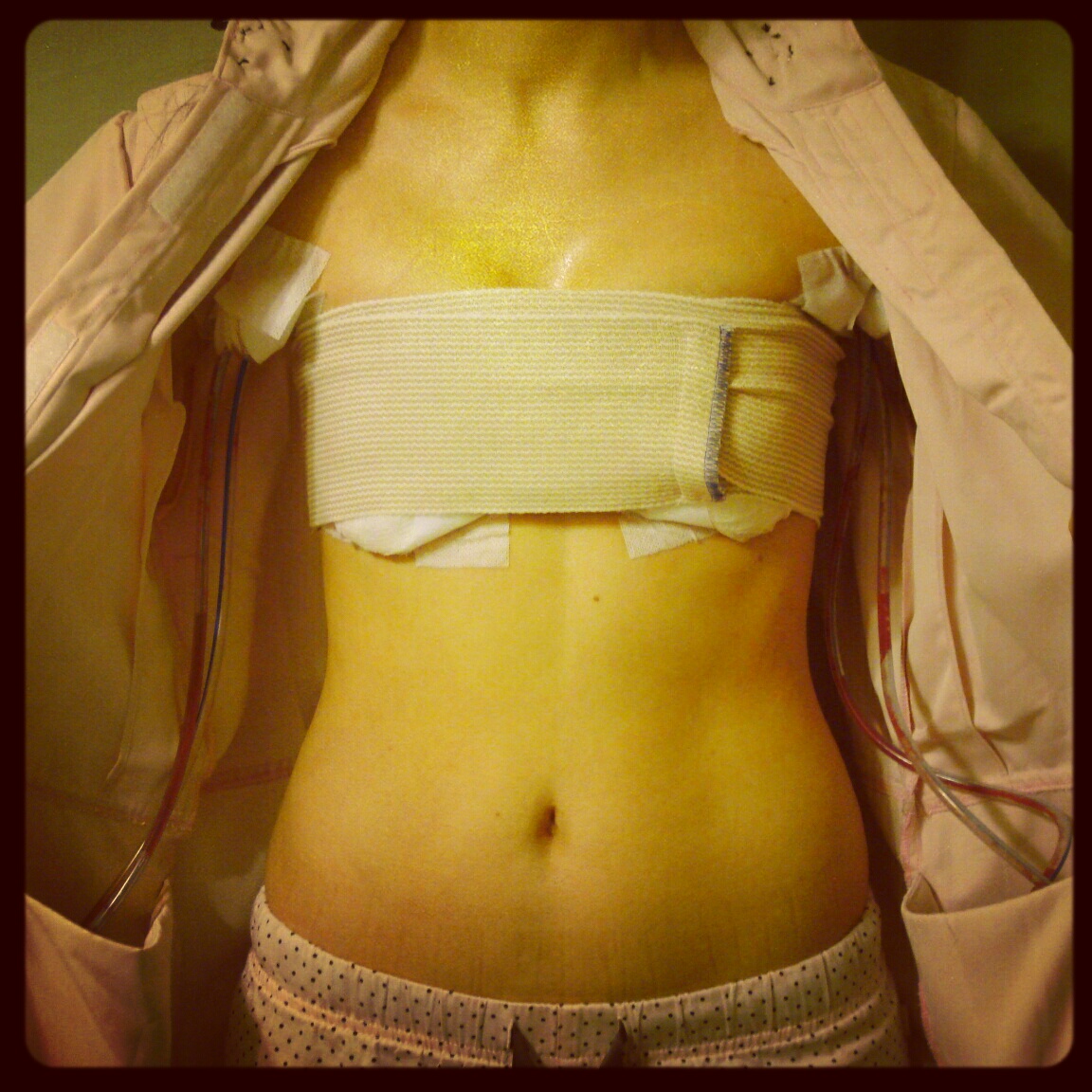
I put on the super-awesome gown that was dropped off by the local Pink Passion Breast Cancer Support Group coordinator. It opens in the front, has flaps on each side of the chest for easy access, and has huge inside pockets to hold the drains. The hubby got the car warmed up and brought it to the front door, where I was taken in a wheelchair by one of the nurses.
Finally home
Borrowing a recliner is the best thing I did to prep for the recovery. It is an electric one, so I don’t have to pull the lever to use it. It is set up downstairs in the living room, with a bunch of the stuff from my checklist spread out around it. I could rest and sleep comfortably without worrying about turning over in the middle of the night.
Bathroom breaks
Prune juice
Getting the medication dosage and timing right took a couple of tries, but once I got it nailed down, I was doing great. The trips to the bathroom decreased since I was off the IV, but I made it a point to try to go every four hours when I woke up for meds. I was conscious of the fact that I hadn’t gone #2 yet, but not freaking out. Since the stool softener (Colace) was the only thing that got me nauseous, I stopped taking it and started downing Sunsweet Prune Juice. This worked! Also, each time I got up, I took at least two laps around the house to get the blood flowing.
Drain management
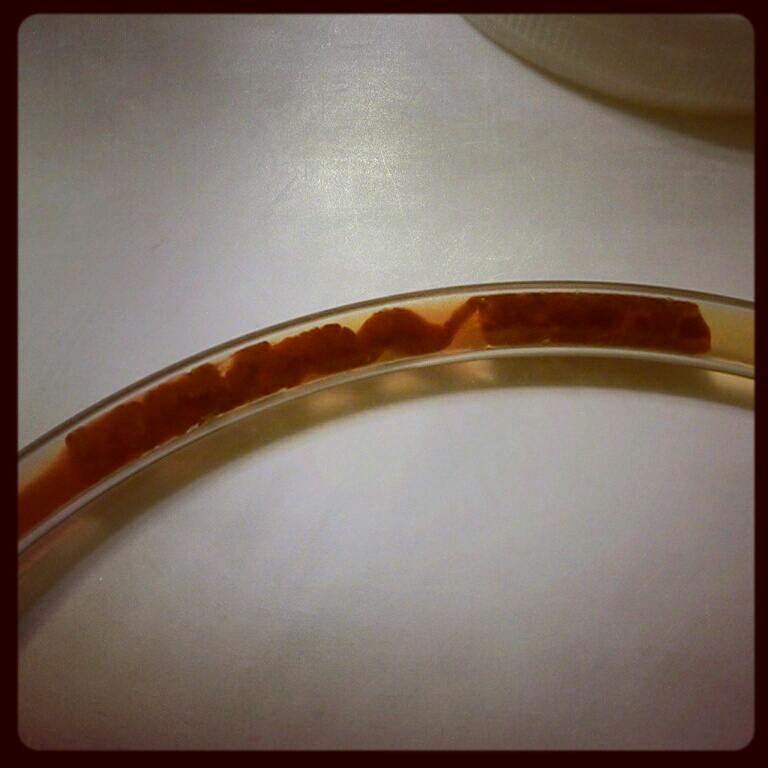
Emptying the drains was a bit overwhelming at first, but became just a normal thing we had to do. Hubby and I did this two times per day. Gear: rubber gloves, alcohol swabs, measuring cups, note pad, and pen. Each reservoir was emptied, the volume recorded, the port/hole wiped with an alcohol swab, the drain “charged,” and the fluid flushed down the toilet. The drain tubes were interesting (one might also use the word “gross”) to look at. There were clots visible in the lines, but not a problem. The fluids kept draining, so everything was good.
Clot
More fun stuff coming next, but first, an important announcement from Grumpy Cat, a.k.a. Tardar Sauce.
All that’s left to do now is to get through the items on my Preparing for surgery list, think positive, and avoid getting sick! It just got real. It’s the final countdown.
Went to see the plastic surgeon for the last pre-op appointment. We discussed a few last details:
Some ladies are told not to shave, as it may increase chance of infection. Is shaving OK before the surgery? Yes, it’s fine.
Will I get a pain pump implanted or IV-type pain medication while at the hospital? The pain medication will be administered via IV, not a pump. Implanting the pump creates additional surgical/wound sites and isn’t necessary for this type of procedure.
How soon after surgery do I start follow ups? I will meet with the surgeons before leaving the hospital. If there are issues after leaving, may see the plastic surgeon every day, may not see him for a few days. Depends on how things go. Will keep in touch.
How soon will the first MRI need to be completed? The MRI is done two years after the implants are in, so nothing to worry about in the immediate future (especially since this will be a staged reconstruction, which means the final exchange of implants for expanders will not take place until about six months after mastectomy). These screenings will be monitored by the plastic surgeon. Breast cancer screenings will continue via clinical exams from the breast surgeon/OB-GYN/PCP.
Is physical therapy recommended? Not typically. Some women are back to normal fast, some take a few weeks. Try to do things without help from others (within reason). Brush your own hair the day you get back from the hospital. When you can shower, wash your hair yourself. Do some range of motion exercises. If not making progress, PT may be recommended to help with the recovery.
Added 1/19: Check out this awesome video from Casey Eischen, BS, CSCS, CPT, CES, Health/Fitness Expert and Nutrition Coach, providing levels 1 & 2 of a great exercise program for women who have undergone a prophylactic bilateral mastectomy. More to come!
Exercises to Recovery from Phophylactic Mastectomy/Reconstruction
I met with Dr. K to talk about a few things I wanted to revisit before we sealed the deal. One of them being: whether or not my mastectomy will be nipple-sparing (see Nipples, pecs, bras, OH MY!). Some of the things we talked about:
How much breast tissue (if any) will be left behind? A small disk of breast tissue remains under the nipple to prevent inversion.
What are the chances of breast cancer diagnosis? In the case of a prophylactic mastectomy (especially for a BRCA1/2-mutation-negative patient), the risk of developing breast cancer is still very low (<1%; see this summary table from the related article mentioned below). A long-term Georgetown study (related article #2 below) concludes that nipple-sparing mastectomy can be safe in properly selected patients.
What type of screening is done long-term? Screening is still required after any type of mastectomy via self and clinical exams. Mammography/ultrasounds/MRIs are generally not needed. However, screening MRIs are required when breast implants are used for reconstruction.
What are the chances of necrosis? From the nipple-sparing mastectomies my breast surgeon has performed, no nipples have been lost. He will make the incision laterally from the edge of the areola, versus circumareolar (tracing around it and then out). This will make the procedure technically a bit more difficult, due to a smaller access hole to the cavity, but will reduce the risk of necrosis. The article mentioned below also provides some data related to necrosis of the nipple-areola complex. 2/9: The incision that was actually made was a curved/smiley-face line about two inches below my nipple.
Will I have any feeling left? This is unlikely. Nipple(s) can become erect after this type of procedure, but the experience will not be the same as pre-mastectomy, both in cause and sensation.
So will I have permanent headlights? This is a possibility. A few of the ladies I’ve spoken to have expressed that this is true for them after a nipple-sparing procedure. As you can imagine, having constantly-erect nipples can make things awkward, so definitely something I hope I don’t have to deal with. However, in discussing with my PS, I learned that as with other possible unsatisfactory results, it can be addressed in a few different ways. Worst case scenario: another procedure to remove the nipples and areolae.
I’m confident that Dr. K is technically capable of performing this type of procedure and will do a great job. I am aware of the potential complications (not all listed here) – we’ll cross that bridge if we get to it.
Whew, that was the last thing to mull over, last detail to plan, last thing on my list that’s up to me (well, this list). Now the breast surgeon’s office confirms the insurance pre-authorization and I sign the consent forms. One pre-op appointment left with my plastic surgeon.
I visited my plastic surgeon again to get a few more questions answered. Among them: what are we going to do with these nipples? I’m still waffling over keeping them and doing nipple reconstruction later. The reasons this is so difficult for me are many.
If they stay:
Will they die? Will they be in the right spot on my reconstructed breasts? What will the proportion be to my new breast size? Will I have any feeling left? Will I have permanent headlights? Basically, keeping the nipples intact leaves a few things up to chance. If the surgeon does a spectacular job and doesn’t snip any nerves or vessels that are essential to survival, we’re good; if something goes wrong, more surgeries will be needed.
If they go:
How much bigger will the scars be? Will I miss them? Will my husband be put off? How long until I can get some nipples back on these babies? Will the breast shape lose some projection and look a bit flat? Will I get 3D tattoos or something more creative? This seems like the less complicated route and nipple reconstruction is an option.
The plastic surgeon and I discussed these concerns and options. He did note that for each woman that undergoes a mastectomy as a preventative measure, about 30 are doing it after a cancer diagnosis. Saving the nipples is not a very safe choice once there are cancer cells in the body, therefore some surgeons don’t have much experience with nipple-sparing mastectomies. Out of the patients my plastic surgeon has worked with, there have been zero nipples lost. However, he is not the one that will be wielding the scalpel when the incisions are made. That lies in the hands of the other surgeon. When I recently met with him (see Speed Bump), he didn’t seem too keen on the nipple-sparing route. I am withholding making the call until I meet with him again and discuss this in more detail.
Other questions from this visit with plastic surgeon:
Do we really need to snip the pec nerves? NOT doing it isn’t really an option. It is done to create the pocket, but also for optimal projection. If the pec major remains completely intact (not sure this is even possible), this can cause “jumping boob” when you shake hands, reach for things, or even have a conversation, if you talk with your hands.
Will I have to wear a bra (ever)? No. I just want to take a second here and say “woo hoo!!!“ There will be an ace bandage wrapped around the chest for at least a couple of days post-surgery, but long-term a bra is not needed. Side note: As women age, they typically gain weight and the different types of tissue that make up the breast lose elasticity, so everything starts drifting south due to gravity. All of that tissue is removed during the mastectomy. Also, a piece of AlloDerm is implanted under the skin and acts as a sling for the breast implant (check out this 2 min video on YouTube – NSFW). Want a laugh? Check out this lady whose boobs sagged so low she just tucks them into her pants!
Should I use BioOil before and after surgery to soften tissue and minimize scars? Maderma and other products that help reduce scars are a waste of money. The most effective way to do this is to stimulate the tissue by applying pressure to it. One hour each day, take some “me” time and massage the scar tissue on the breasts.
Will you be performing the entirety of the reconstruction?Meaning: will any medical students/residents be practicing on me? Residents may be present to watch the surgery, but they do not participate. A surgical assistant will the stitching after everything is done.
When do you submit for insurance pre-authorization and does the general or the plastic surgeon complete the disability paperwork? The breast surgeon does his pre-authorization first, then the plastic surgeon submits the paperwork. Disability paperwork is completed by the plastic surgeon about three weeks out. By the way, the Women’s Health and Cancer Rights Act of 1998 (WHCRA) requires insurance companies covering the mastectomy to provide coverage for all stages of reconstruction of the breasts and treatment of physical complications of the mastectomy (doesn’t matter if prophylactic). Note: this is IF the insurance company covers the mastectomy.
So what’s actually going to happen? How does this work?
The prophylactic bilateral mastectomy is serious business. The operation can range from four to over 12 hours – depends on what type of mastectomy (skin-sparing, nipple-sparing) and reconstruction (direct, delayed, implant, DIEP, TRAM, other flap, fat transfer) are planned. It requires at least one night’s stay in the hospital and has a lengthy recovery (multiple-week’s-worth, not just a few days). During a mastectomy the surgeon removes all of the breast tissue leaving little or none behind. The breast reconstruction can happen or begin at the same time the breast tissue is removed: the breast surgeon removes the tissue and hands off the scalpel to the plastic surgeon who does his magic.
After consulting with both surgeons, I chose to have a skin-sparing mastectomy and go the two-stage implant route for reconstruction. Sadly (or not – depends on how you look at it) I do not have enough extra tissue and fat to spare for some new boobies. I’m still undecided on whether or not I want to keep my own nipples, but more on that later.
This whole procedure scares the crap out of me. Even though I’m still two months out, I’m already nervous! There are so many things that need to be considered and so many unknowns. A few things are still up for discussion with the surgeons. I have another list going and will be meeting with both of them again to get some more info to help me decide (updated a couple of answers post-appointment).
Do we need to biopsy the sentinel node to see what’s going on there? Original verdict was no, but to be re-discussed with new surgeon (see Speed Bump). The answer is still no.
Should I keep my nipples? Eventually decided that I’m going to keep them.
Do we really need to snip the pec nerves? It is done to create the pocket, but also for optimal projection. If the pec major remains completely intact, this can cause “jumping boob” when you shake hands, reach for things, or even have a conversation, if you talk with your hands.
When do we do insurance pre-authorization? Breast surgeon does it first about a month before surgery. Plastic surgeon submits after that is granted.
How long will I be unable to shower, open my own water bottles, high-five, do the nasty, drive, work, etc.?Timetable for Healing is one of the sections in the Breast Reconstruction Guidebook and details the first four weeks post-mastectomy. You are back to most of your normal routine during week four.
Aside from worrying about infections and other surgery complications, the thing that bugs me most is long-term limitations on physical activity. During the procedure, the surgeons snip some of the nerves that are attached to the pectoralis major to create a pocket for the implant. Because of this, the pec major atrophies and loses some of it’s function. The pec minor learns to pick up the slack, but doesn’t fill the shoes. Does this mean that I won’t be able to go rock climbing again? How about wake boarding? Eek! Anyway, another topic to research and discuss.
I made appointments for consults with the three plastic surgeons. Not being too familiar with the procedure, I made a list of the questions that immediately popped into my head. Then I made Google my new best friend. After many hours online and a ton of information and photos, most of my general questions were answered. I narrowed it down to the ones that were more specific for me (I now know the answers, so including them as well):
Which procedure would be best for me? Nipple-sparing bilateral mastectomy with two-stage breast reconstruction.
What are the risks for that type of procedure? Nipple or breast tissue necrosis, infections, seroma, capsular contracture – NSFW, ruptures, rippling, cosmetic issues.
Can I see before-and-after photos of previous patients/work?
What is the time frame for the whole process, from start to finish? Up to six months if there are no serious complications.
Which hospital?
What would be expected of me? Get educated, prepare self and home for recovery, focus on the positive.
What are the surgeon’s qualification and experience?
The point of the consults was to determine who I would like to work with if I wanted to move forward. I remember thinking “How can I decide based on a 30 minute conversation? What should I really consider?” I met with all three of the surgeons recommended. After talking it over with my husband and doing some more Googling, I decided I wanted to work with Dr. M. I based this on a bunch of different things including years of experience, the details we discussed, his demeanor, our “chemistry,” the before-and-after photos of his patients (many binders of them), and the fact that he is well known for DIEP flap reconstruction, which is very complicated and requires microsurgery, so this one should be easy, right?
I already had a breast surgeon, I just picked the plastic surgeon, now all I needed to do was to schedule it.
 Will I be required to wear any type of bra (compressions or underwire) after the exchange surgery? Should I purchase something? No. If any type of compression is needed it will be via ace bandage and dressings or a mastectomy bra that will be issued by the hospital.
Will I be required to wear any type of bra (compressions or underwire) after the exchange surgery? Should I purchase something? No. If any type of compression is needed it will be via ace bandage and dressings or a mastectomy bra that will be issued by the hospital.


 So will I have permanent headlights? This is a possibility. A few of the ladies I’ve spoken to have expressed that this is true for them after a nipple-sparing procedure. As you can imagine, having constantly-erect nipples can make things awkward, so definitely something I hope I don’t have to deal with. However, in discussing with my PS, I learned that as with other possible unsatisfactory results, it can be addressed in a few different ways. Worst case scenario: another procedure to remove the nipples and areolae.
So will I have permanent headlights? This is a possibility. A few of the ladies I’ve spoken to have expressed that this is true for them after a nipple-sparing procedure. As you can imagine, having constantly-erect nipples can make things awkward, so definitely something I hope I don’t have to deal with. However, in discussing with my PS, I learned that as with other possible unsatisfactory results, it can be addressed in a few different ways. Worst case scenario: another procedure to remove the nipples and areolae. Other questions from this visit with plastic surgeon:
Other questions from this visit with plastic surgeon:

