Wondering what a nipple delay is? I was too! I hadn’t heard of this procedure until Angelina Jolie announced to the world that she underwent a prophylactic double mastectomy and this procedure was part of the process.
Since that announcement, many different articles and opinions have been published. A lot of them positive, but a few negative. That’s another post for another day. A few pieces did provide more information on the nipple delay procedure.
 What is nipple delay?
What is nipple delay?
During the nipple delay procedure, the surgeon makes an incision in the skin and severs the breast tissue and blood vessels directly beneath the nipple (it remains attached to the surrounding skin). Due to this, the nipple is no longer dependent upon the blood supply directly beneath it and becomes accustomed to getting its blood supply through the skin. According to the Pink Lotus Breast Center blog, it actually recruits additional blood flow not previously established.
This is an uncommon procedure. If it is elected, it is performed some time before the mastectomy; two weeks for Angelina Jolie.
Why have a nipple delay?
Surgical nipple delay is used to decrease likelihood of nipple necrosis, which can occur because of loss of blood supply and can lead to nipple loss, following a nipple-sparing mastectomy.
Breast skin is fragile after mastectomy. If it’s exceptionally thin after the breast tissue is cut away or is handled too roughly, it may die. The same result may occur if the breast surgeon severs too many blood vessels that feed the skin or uses eletrocautery too aggressively and burns the inside of the skin, which may then blister and die.
– Steligo, Kathy. Breast Reconstruction Guidebook: Issues and Answers from Research to Recovery. Maryland: The Johns Hopkins University Press, 2012. Print, third edition.
I was not informed of this option prior to my own nipple-sparing mastectomy. My compromised blood flow resulted in necrosis on my left breast and I lost a nipple. If you are interested in reading about my bout with necrosis (including photos) and the hyperbaric treatment I underwent in an effort to thwart it, please read Tissue necrosis.
Related articles:
- Surgical Delay of the Nipple–Areolar Complex: A Powerful Technique to Maximize Nipple Viability Following Nipple-Sparing Mastectomy (annsurgoncol.org)
- Angelina Jolie’s ‘nipple delay’ procedure, explained (NYmag.com)
- A patient’s journey: Angelina Jolie (PinkLotusBreastCenter.com)
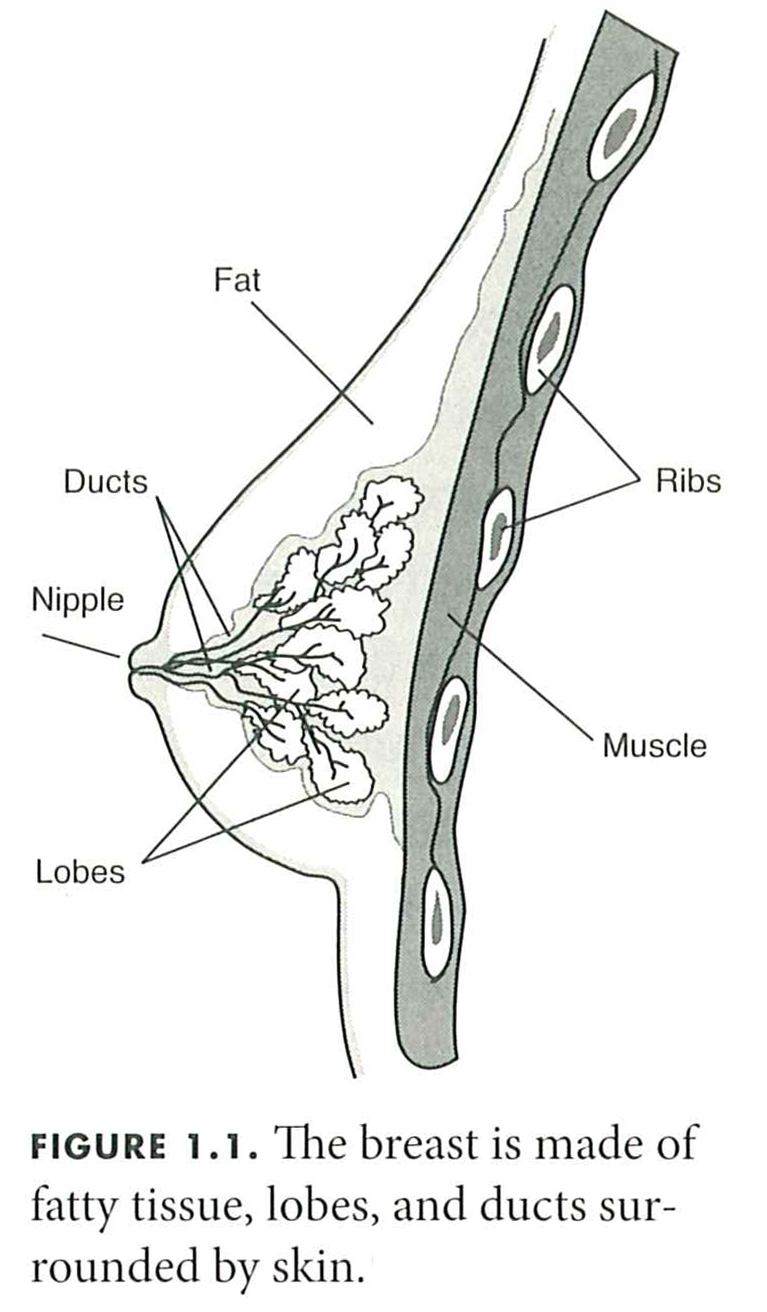
Source of Figure 1.1: Steligo, Kathy. Breast Reconstruction Guidebook: Issues and Answers from Research to Recovery. Maryland: The Johns Hopkins University Press, 2012. Print, third edition.




 How much breast tissue (if any) will be left behind? A small disk of breast tissue remains under the nipple to prevent inversion.
How much breast tissue (if any) will be left behind? A small disk of breast tissue remains under the nipple to prevent inversion. So will I have permanent headlights? This is a possibility. A few of the ladies I’ve spoken to have expressed that this is true for them after a nipple-sparing procedure. As you can imagine, having constantly-erect nipples can make things awkward, so definitely something I hope I don’t have to deal with. However, in discussing with my PS, I learned that as with other possible unsatisfactory results, it can be addressed in a few different ways. Worst case scenario: another procedure to remove the nipples and areolae.
So will I have permanent headlights? This is a possibility. A few of the ladies I’ve spoken to have expressed that this is true for them after a nipple-sparing procedure. As you can imagine, having constantly-erect nipples can make things awkward, so definitely something I hope I don’t have to deal with. However, in discussing with my PS, I learned that as with other possible unsatisfactory results, it can be addressed in a few different ways. Worst case scenario: another procedure to remove the nipples and areolae.