WARNING: NSFW / graphic content below.
Alright boys and girls .. I think we did it! I think we’ve finally arrived at the end. My exchange surgery was on Thursday, September 11. I had pocket revision on my right side and a swap from tissue expander to implant on my left.
 We arrived at the hospital at 6:30am for the 8:30am procedure. It was a beautiful morning! The surgery lasted three and a half hours – longer than we expected. I woke up bundled up in a tight compression bra and ACE bandage wrapped about my chest. The biggest and most wonderful surprise: NO DRAINS!!! I couldn’t believe it. Spent a bit in the recovery room and then hightailed it home to my comfy bed.
We arrived at the hospital at 6:30am for the 8:30am procedure. It was a beautiful morning! The surgery lasted three and a half hours – longer than we expected. I woke up bundled up in a tight compression bra and ACE bandage wrapped about my chest. The biggest and most wonderful surprise: NO DRAINS!!! I couldn’t believe it. Spent a bit in the recovery room and then hightailed it home to my comfy bed.
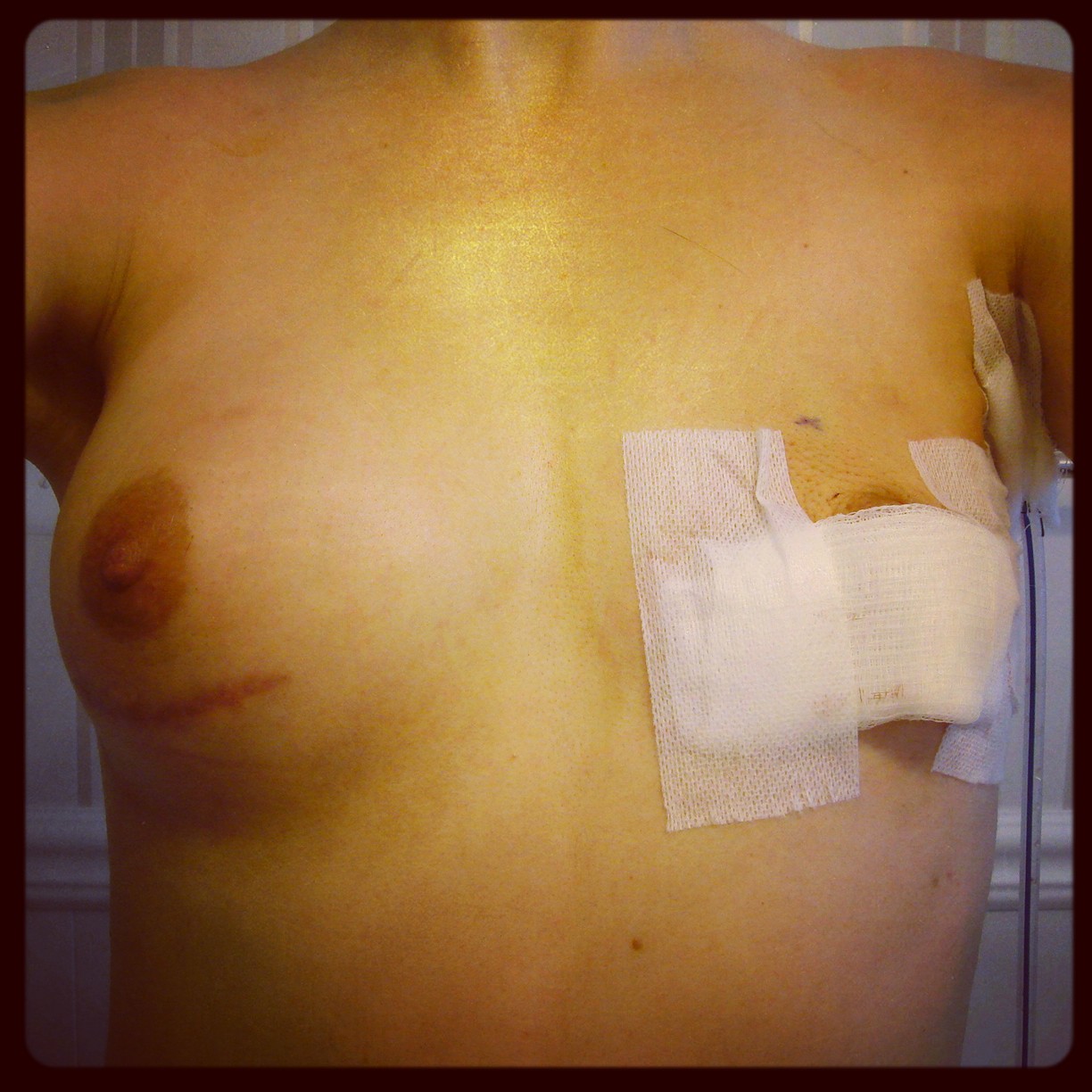
On Friday, we drove out to Dr. M’s office for my follow up appointment, which is when I got to see them for the first time after surgery. Things are looking good! I do have some swelling, which is to be expected, but aside from that they look to be the same size, are even on my chest wall, and my nipples line up. Woo hoo! I know it’s early, as it takes up to a year for things to settle, but I am just ecstatic!

Dr. M explained what he found while he was in there. It appears that at some point since my last surgery in April I ripped apart the pocket revision he did then and this is why the right side was bottoming out again. This could’ve happened as I bumped into something or fell or had some other physical strain or trauma. Hub pointed out that it may have something to do with me painting. Yes, I admit, I did more than I should have. I’m an idiot. This time around I am doing N O T H I N G. Absolutely nothing. For at least a month. And no excuses!
On my left side, Dr. M made the incision underneath the nipple, where the original was, rather than going in through my armpit again. He had to do some work on that side to make sure symmetry was achieved, hence a bit more swelling there. He did not do any fat grafting, which made me happy and I did stay with the same implant size and projection I had previously: Mentor round, smooth, high profile, silicone in 450ccs.
I am feeling amazing! I think the girls look great and physically I am not in too much pain. I am to wear this compression bra for two weeks straight, with the exception of showering. This will ensure everything heals in place as it should. Next appointment: September 25.


 Nipple symmetry – the left nipple became
Nipple symmetry – the left nipple became 


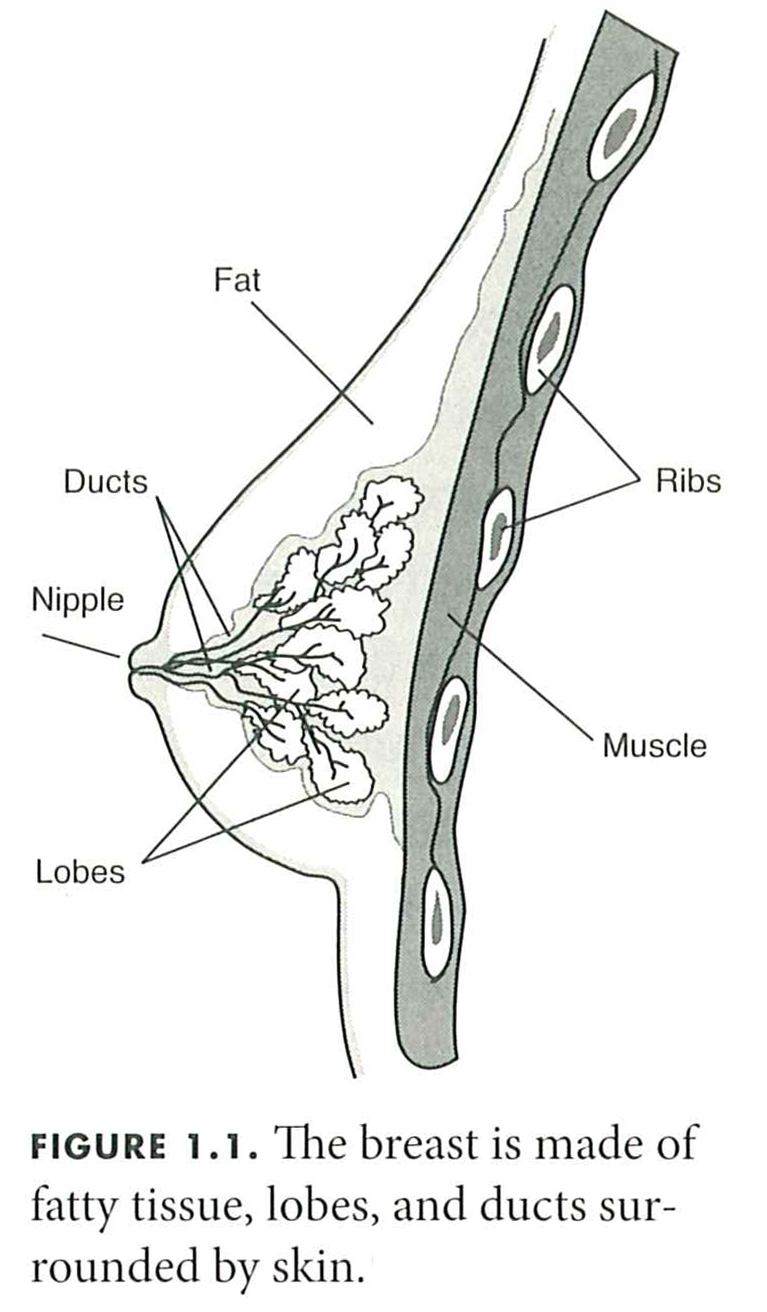
 Breast skin is fragile after mastectomy. If it’s exceptionally thin after the breast tissue is cut away or is handled too roughly, it may die. The same result may occur if the breast surgeon severs too many blood vessels that feed the skin or uses eletrocautery too aggressively and burns the inside of the skin, which may then blister and die.
Breast skin is fragile after mastectomy. If it’s exceptionally thin after the breast tissue is cut away or is handled too roughly, it may die. The same result may occur if the breast surgeon severs too many blood vessels that feed the skin or uses eletrocautery too aggressively and burns the inside of the skin, which may then blister and die.
 I have a desk job, so it isn’t very physically demanding, but I did feel completely pooped after my second day back. Sitting in one spot for most of eight hours is much different than lounging on the couch and it caught up with me. I find that the tightness across my chest, while not painful, is uncomfortable, so my shoulders droop to relieve the pressure and I slouch. Although I’m more comfortable that way, it makes my whole body ache at the end of the day. It’s just awkward. I must admit that I was getting kind of bored at home, though, so the return to work was good for me. I missed the face-to-face interaction with my friends and co-workers.
I have a desk job, so it isn’t very physically demanding, but I did feel completely pooped after my second day back. Sitting in one spot for most of eight hours is much different than lounging on the couch and it caught up with me. I find that the tightness across my chest, while not painful, is uncomfortable, so my shoulders droop to relieve the pressure and I slouch. Although I’m more comfortable that way, it makes my whole body ache at the end of the day. It’s just awkward. I must admit that I was getting kind of bored at home, though, so the return to work was good for me. I missed the face-to-face interaction with my friends and co-workers. Hyperbaric oxygen therapy (HBOT) involves the breathing of pure oxygen while in a sealed chamber that has been pressurized at 1-1/2 to 3 times normal atmospheric pressure. –
Hyperbaric oxygen therapy (HBOT) involves the breathing of pure oxygen while in a sealed chamber that has been pressurized at 1-1/2 to 3 times normal atmospheric pressure. – 




