WARNING: NSFW / graphic content below.
Before I tell you about what has been happening for the last few days, I just want to say to those that are considering this procedure, preparing for one, or have already started the process: women who undergo a mastectomy, whether prophylactic or not, don’t always experience complications. Actually, I’d say that most do not, based on my involvement in a few online support groups and interaction with women in my local community. Everybody’s experience is different, because of different doctors, hospitals, body condition, other health issues, activities during recovery, nutrition, etc. There are many factors. Each person should consider their scenario and discuss concerns they may have with their surgical team.
Another thing to keep in mind is that usually the people that have problems are the ones that speak up. You know – the squeaky wheel thing. There are so many women out there that have had a completely complication-free experience and have beautiful results! You can’t tell that they’ve gone through this journey unless they tell you! Those women usually don’t linger in the support groups, stop blogging about it, move on, and just leave it all behind them. They are DONE and don’t have to think about it again.
Okay, Houston, we’ve had a problem here
Unfortunately, I’m not one of them. Upon my return from vacation, I started working out again (cardio) and I also began using Kelocote on my hypertrophic scars, as I mentioned in a recent post. Both of these activities began on Sunday. The following Wednesday I saw Dr. M and things looked good. The next day I noticed a bit of redness around the incision on my left breast. By Saturday there was a small area in the center of the scar tissue from my bout with necrosis that had turned blue. I emailed Dr. M and got this response:
Yes, this is a significant problem. Need to see you tomorrow.
 By Monday afternoon, I had a hole. By early evening I had chills, sweats, and a fever of 101.7. Panicked, I called the after-hours service to page Dr. M and he called back immediately. The plan was to continue on the antibiotics, take a couple Tylenol, and sit tight unless the temperature spiked past 103, at which point I’d hightail it to the ER. Within two hours the temperature dropped below 100, but I knew what was coming: the implant had to go.
By Monday afternoon, I had a hole. By early evening I had chills, sweats, and a fever of 101.7. Panicked, I called the after-hours service to page Dr. M and he called back immediately. The plan was to continue on the antibiotics, take a couple Tylenol, and sit tight unless the temperature spiked past 103, at which point I’d hightail it to the ER. Within two hours the temperature dropped below 100, but I knew what was coming: the implant had to go.
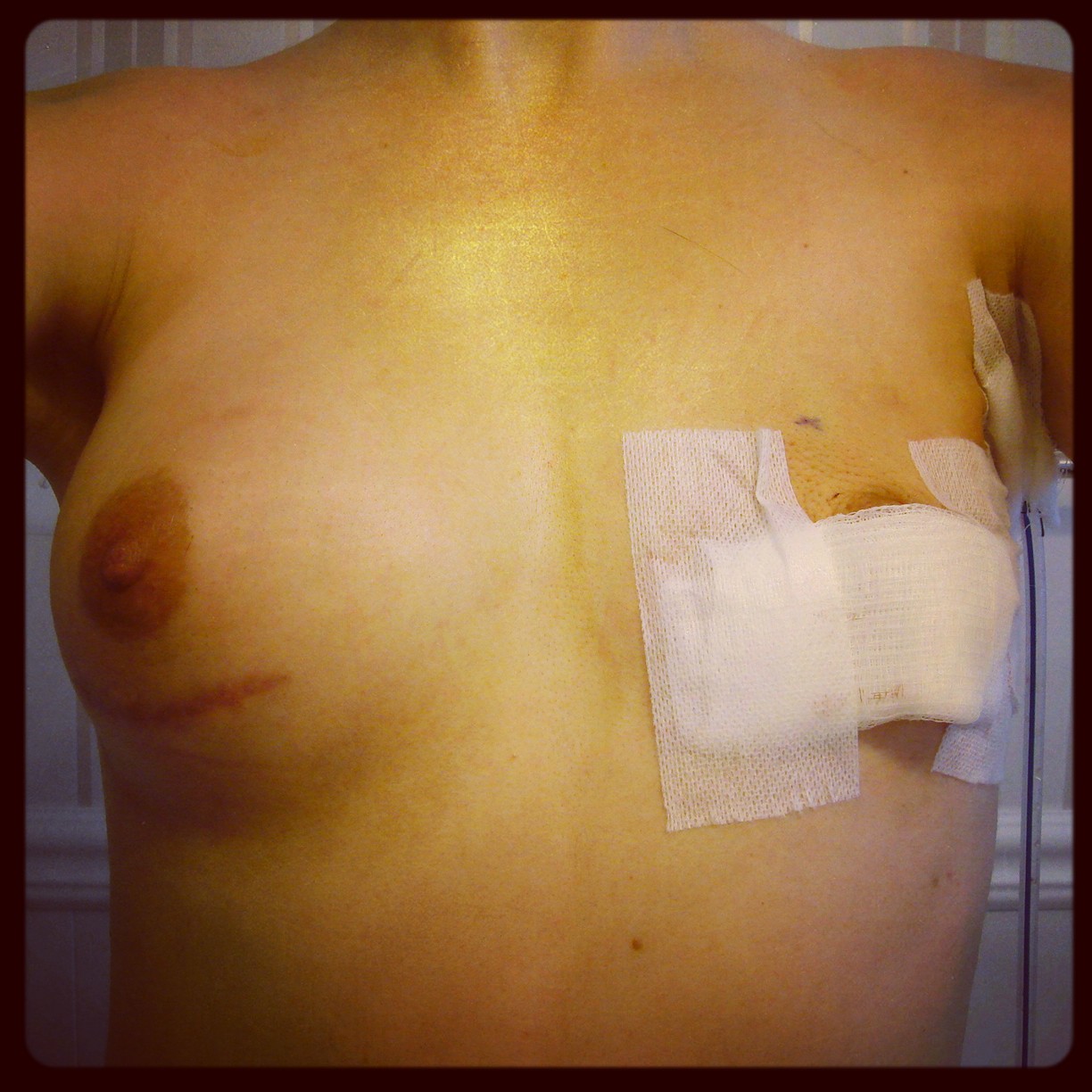
My surgery was at 5pm on Tuesday, October 15. Dr. M cleaned up the incision and removed the implant. I am left with one breast and another drain! I really REALLY don’t like drains, but who does? What’s next? We have to let everything heal for at least three months before we being talking about restarting reconstruction on that side. I’m am so bummed by this humongous setback!
Why did this happen?
A combination of things may have caused this, but it’s hard to say exactly which was the straw. In Dr. M’s experience, implants are usually (but rarely) lost due to complications from three major things: radiation, smoking, and/or trauma. I fall into the third category. The necrosis I experienced in January produced a lot of scar tissue, which has poor circulation. My use of Kelocote on that scar tissue introduced chemicals into the equation. On top of that, I started working out again. My body protested against the combination of old and new trauma. So here I am, uniboobin’ it for at least three more months! Good thing it’ll be during winter and I can camouflage things a bit. I present a foob and a drain:
 Hyperbaric oxygen therapy (HBOT) involves the breathing of pure oxygen while in a sealed chamber that has been pressurized at 1-1/2 to 3 times normal atmospheric pressure. –
Hyperbaric oxygen therapy (HBOT) involves the breathing of pure oxygen while in a sealed chamber that has been pressurized at 1-1/2 to 3 times normal atmospheric pressure. – 


 Breast skin is fragile after mastectomy. If it’s exceptionally thin after the breast tissue is cut away or is handled too roughly, it may die. The same result may occur if the breast surgeon severs too many blood vessels that feed the skin or uses eletrocautery too aggressively and burns the inside of the skin, which may then blister and die.
Breast skin is fragile after mastectomy. If it’s exceptionally thin after the breast tissue is cut away or is handled too roughly, it may die. The same result may occur if the breast surgeon severs too many blood vessels that feed the skin or uses eletrocautery too aggressively and burns the inside of the skin, which may then blister and die.

